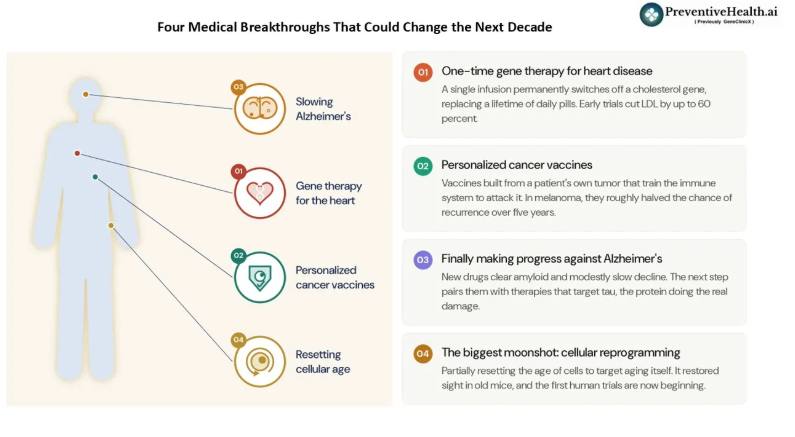
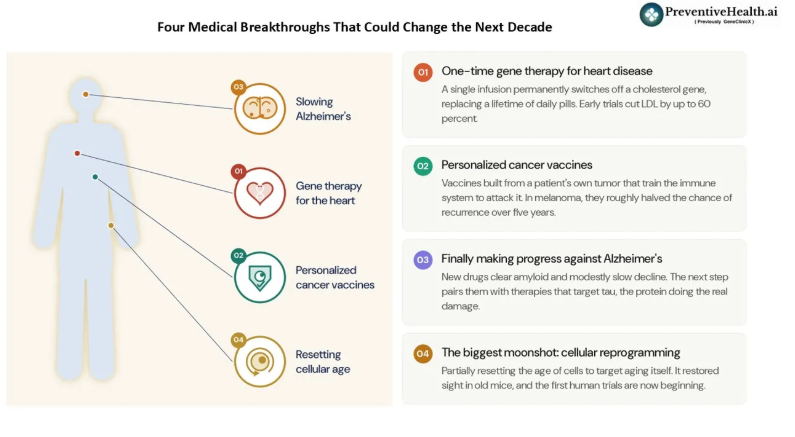
What are the most exciting advances in medicine on the horizon, the ones that could prevent or treat our biggest killers like cancer, heart disease, neurodegenerative disease, and metabolic disease? New studies appear every day, but a few stand out. In today’s post (#75), I cover four that are still early but scientifically plausible, and that the leading research institutions are watching with cautious optimism. All four are still working their way through clinical trials, and medicine is full of promising ideas that never reach the finish line, so some realism is in order. But if I had to pick the breakthroughs most likely to change human health over the next decade, these would be near the top of my list.
1. A one-time gene therapy for heart disease
Heart disease remains the leading cause of death worldwide. For decades, the standard approach has been simple: identify people with elevated cholesterol and give them medications such as statins. The medications work, but they only work if people take them consistently for decades.
What if one treatment could replace a lifetime of pills? There is a gene called PCSK9 that is primarily active in the liver, that contains the instructions for making the PCSK9 protein. This protein limits the liver’s ability to remove LDL cholesterol, often called “bad cholesterol” from the bloodstream. Researchers are now developing gene-editing therapies that permanently switch off this PCSK9 gene in the liver.

The whole idea came from people born this way. Researchers found rare individuals with both copies of PCSK9 naturally switched off. A very good friend of mine has this mutation and consequently has an LDL of 26 mg/dL (should be lower than 100 mg/dL); he is 50+, lives an average lifestyle, and isn’t on statins. People like him tend to have dramatically lower rates of heart disease, and their biology became the blueprint for the drug. We already have PCSK9 drugs that neutralize the PCSK9 protein in the blood, but they are injections taken every few weeks for life. The goal is to recreate that natural protection through a single infusion that changes one letter of DNA in the liver, and permanently switches off production of the PCSK9 protein.
The early human results are striking. In a 2026 trial, a single infusion lowered LDL cholesterol by as much as 60 percent. That is on par with the best cholesterol-lowering drugs we have today. And the effect has held steady for well over a year in the patients followed so far, which is exactly what you would want from a one-time treatment. If these therapies continue to prove safe and durable in larger studies, we may eventually reach a point where a person receives a single treatment in their 30s or 40s and carries lower cardiovascular risk for decades. That is a very different future from taking daily medication for the rest of your life.
2. Personalized cancer vaccines
The word “vaccine” usually makes us think about preventing infections. However, cancer vaccines work differently. Every cancer contains mutations that make it unique. Scientists can now sequence a patient’s tumor, identify those mutations, and create a personalized vaccine designed specifically for that individual’s cancer.
There is a puzzle at the heart of this. If cancer is so dangerous, why doesn’t the immune system already destroy it? The problem is that cancer cells are not foreign invaders. They are your own cells that have gone wrong, so the immune system tends to treat them as friendly and leaves them alone. That is what lets a tumor grow unnoticed.
A vaccine personalized to an individual’s tumor solves that puzzle. When a cell turns cancerous, its mutations cause it to produce tiny abnormal proteins that appear nowhere else in the body. The vaccine carries the fingerprints of those proteins and shows them to the immune system, in effect saying, this is what the enemy looks like, go find it. Because those fingerprints are unique to the tumor, the immune system can attack the cancer while leaving healthy cells untouched. This is personalized medicine in the truest sense, since two people with the same type of cancer may receive completely different vaccines.
Some of the most promising results have emerged in melanoma (a type of skin cancer) and pancreatic cancer. In melanoma, adding a personalized vaccine to standard immunotherapy roughly halved the chance of the cancer returning over five years. In pancreatic cancer, one of the hardest cancers to treat, six-year follow-up showed that most patients whose immune systems responded to the vaccine were still alive. These are small, early studies and are expected to be expanded to the other cancers over the coming years.
3. Finally making progress against Alzheimer’s disease
Alzheimer’s disease has been one of the most frustrating challenges in modern medicine. For nearly thirty years, almost every drug aimed at the disease failed. That long graveyard of failures is why even modest progress now feels like a turning point.
To understand the progress, it helps to know what actually goes wrong inside the brain. Two proteins are the main culprits. The first is amyloid, a sticky substance that builds up in clumps between brain cells, like hardened plaque collecting on the outside of the neurons. The second is tau. Tau normally lives inside the neuron, where it forms the scaffolding that holds the cell’s internal transport system together. In Alzheimer’s, that scaffolding collapses into tangles, and the cell slowly strangles from the inside.
For years, the entire field bet on amyloid. The thinking was that if you could clear away the sticky plaques, you could stop the disease. The newest drugs finally proved that you can in fact remove amyloid from the brain, and doing so does modestly slow decline. That was a real milestone, because it showed for the first time that the disease process can be altered rather than simply managed.
But the benefit was smaller than many had hoped, and there is a good reason why. A useful way researchers describe it is that amyloid is the trigger, but tau is the bullet. Amyloid may set the disease in motion, but tau is the protein that does the actual damage to brain cells, which is why tau tangles track far more closely with a patient’s symptoms. Removing amyloid pulls back the trigger, but by the time symptoms appear, the bullet is already in flight.
That is why the next step matters so much. Researchers are now testing therapies that go after both proteins at the same time, clearing the amyloid that starts the process while also breaking up the tau tangles that carry out the damage. Hitting the trigger and the bullet together could do far more than either one alone, and trials testing exactly this combination are now underway.
There is also movement on the prevention side. New blood tests can now flag the disease years before symptoms appear, which is exactly when any future therapy would do the most good. The first, the Lumipulse pTau217 test, was cleared by the FDA in 2025 and is now available through labs like Labcorp, with others close behind. It costs a few hundred dollars, far less than a brain scan. For now these are meant for people already noticing memory problems and are best ordered through a doctor. If successful, Alzheimer’s may gradually become a disease that can be slowed and managed rather than one that relentlessly progresses without meaningful intervention. Given the aging of populations around the world, the implications would be enormous.
4. The biggest moonshot: Cellular reprogramming
Everything we have discussed so far targets a specific disease. Cellular reprogramming is different. It targets aging itself.
To see how, it helps to understand something interesting about your body. Every one of your cells carries the same complete set of DNA, the same full instruction manual. Yet a skin cell, a heart cell, and a brain cell all look and behave completely differently. That is because each cell only reads the pages of the manual that apply to its own job and ignores the rest. The system of chemical “bookmarks” that tells a cell which pages to read is what gives it its identity.
As we age, those bookmarks get smudged and disorganized. Cells gradually lose track of which pages they are supposed to read, and they start to work less well. The breakthrough idea is that we may be able to tidy up the bookmarks and restore a cell to a younger, better-functioning version of itself. The idea comes from the Nobel Prize-winning work of Shinya Yamanaka, who discovered a set of four molecules that can wind a mature cell all the way back to a blank, embryonic state. Reprogramming for aging uses a gentler version of the same trick. The goal is to rewind the clock only partway, restoring youthful function without erasing the cell’s memory of what its function is.
The most striking proof came from the eye. In one landmark experiment, researchers restored sight to old mice, and to mice whose optic nerves had been crushed, by partially resetting the age of the cells in their eyes. Cells that had lost the ability to repair themselves began behaving like young cells again, and vision returned. Tellingly, the researchers used only three of Yamanaka’s four molecules, deliberately leaving out the one most strongly linked to cancer.
That caution points to the central danger. If you reset a cell too far, it does not simply grow younger. It forgets what it was. A skin cell or a liver cell that has lost all memory of its job, and that keeps dividing without restraint, is essentially the definition of a cancer. The whole challenge is to turn the clock back far enough to rejuvenate a cell, but not so far that it loses its identity and turns dangerous.
Before anyone gets too excited, it is worth remembering how early this is. Almost all of the strongest evidence still comes from animals, and the very first human trials are only now beginning, fittingly in the eye, where a treatment can be contained and watched closely.
But if it works, the implications could be unlike anything medicine has ever seen. Instead of treating heart disease, cancer, Alzheimer’s disease, and diabetes separately, we might be able to target one of their most important common drivers: aging itself. That is why many researchers consider cellular reprogramming the ultimate moonshot.
Final thoughts
Whenever we discuss future medicine, it is easy to get carried away. Most experimental therapies fail. Some will prove less effective than expected. Others may encounter safety challenges that prevent widespread adoption. But what excites me about this particular group of technologies is that they are not science fiction. They are grounded in real biology, supported by serious scientific research, and being evaluated by some of the world’s best clinicians and researchers. But if even a few of them succeed, the next decade may look very different from the last. And that is a future worth paying attention to.
Nickhil Jakatdar is the CEO of GenePath Diagnostics and the founder of PreventiveHealth.ai, working to make advanced diagnostics and credible health guidance more accessible, affordable, and actionable. A PhD in EECS from UC Berkeley and the youngest recipient of the UC Berkeley Distinguished Alumnus Award, he has founded and led multiple tech companies. He holds 60 patents, and serves on several academic, healthcare, and innovation boards. To follow his thinking on preventive health, technology, and systems that scale expertise, join his private WhatsApp community and subscribe to his Substack.
Disclaimer
Views expressed above are the author’s own.