Few areas of medicine generate as much fascination, hope, hype, and confusion as genetics. Just over two decades ago, sequencing the first human genome required thousands of scientists working across the globe, more than a decade of effort, and a budget of roughly $3 billion. Today, the same task can be completed in less than 24 hours for under $200.
Most people intuitively understand that DNA is important. After all, it is the biological blueprint we inherit from our parents. Yet despite this extraordinary progress, most people still have only a vague understanding of what genetics or genomics actually is (I explain how they differ below) and why it may become one of the most important tools in preventive healthcare. We are entering an era where understanding our biology is becoming easier and cheaper than ever before. But interpreting it correctly remains incredibly difficult.
This post (#76) grew out of a conversation with my friend and colleague, Dr. Nikhil Phadke, a leading genomics and molecular biology expert, on our community podcast.
Genomics: The instruction manual of life
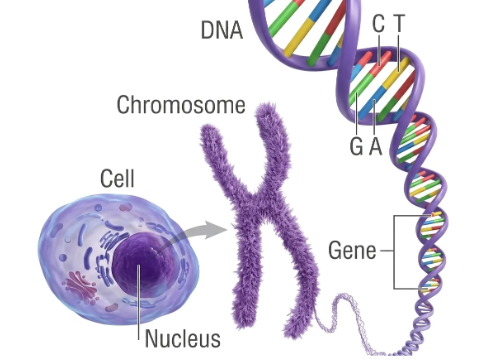
Let’s start with the basics. Your genome is the complete set of instructions for building and running you, written in DNA and inherited from your parents. Two things make it remarkable.
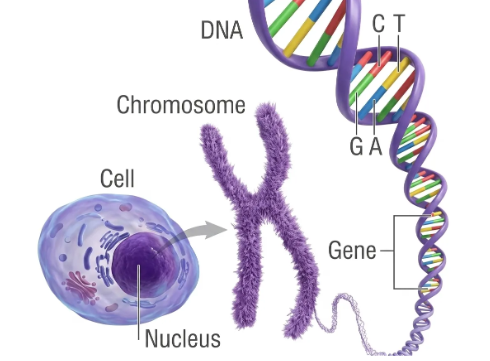

The first is its simplicity. DNA uses just four chemical building blocks, represented by the letters A, T, G and C. Every instruction for life is written in this four-letter code. Within this code are around 20,000 genes. Think of these as recipes, each carrying instructions for making a protein or performing a biological function. These genes are organized into 23 pairs of chromosomes, which you can think of as chapters in a book. Together, they form the complete instruction manual for life.
The second is its size. Your genome is about six billion letters long. If you printed it out as plain text, it would run to roughly the equivalent of a thousand complete Harry Potter series, all seven books, back to back.
Here is the surprise: our genes make up only about 2% of the whole genome. For decades, scientists wrote off the other 98% as “junk DNA,” and it is woven all through the chromosomes, sitting between the genes and even inside them. Picture opening one of those Harry Potter books and finding that only about one word in fifty was part of the story, while the rest looked like gibberish. That is roughly how our DNA once appeared to scientists. We now know that much of the so-called junk is not junk at all. We are still only beginning to understand how it all works.
One more interesting point: any two people are about 99.9% genetically identical. Almost everything that makes you unique is written in the remaining 0.1%. That is all that differentiates you, Nelson Mandela and a serial killer. Side note: Genetics traditionally studied one gene at a time, a sentence here, a paragraph there. Genomics reads the entire manual at once.
Epigenetics: Why your genes are not your destiny
If the genome is the instruction manual, epigenetics is the set of notes in the margins that decides which instructions actually get followed.
Your DNA sequence stays essentially the same your whole life. But the way those genes are read can change dramatically, and that is what epigenetics studies: changes in how genes are expressed without any change to the underlying code.
A simple analogy makes it click. The words “resume” and “résumé” contain exactly the same letters. Add a small accent mark and the meaning changes completely. In this example, the letters are the equivalent of the DNA and the accent is the equivalent of epigenetics. So even if the DNA stays the same, the marks layered on top change how it is read. These marks respond to diet, exercise, stress, sleep, and the environment around us.
The most striking demonstration comes from a strain of mice called agouti mice. Two of these mice can be genetically identical, carrying exactly the same DNA, and yet one grows up lean and brown while the other grows up fat, yellow, and prone to diabetes and cancer. The only difference is what their mothers were fed during pregnancy. Certain nutrients in the mother’s diet add chemical marks that silence a single gene, and that one change reshapes the animal’s coat, its weight, and its lifelong disease risk, all without altering a single letter of DNA. Another reminder that our genes are not our destiny.
Mutations: When a single letter changes everything
A mutation is simply a change in the DNA sequence, a typo in the instruction manual, caused during cell division, or by external factors like radiation or chemicals . Humans carry two copies of most genes, one from each parent. So the effect of a mutation can depend on whether one or both copies are changed. Most mutations are harmless and just add to the normal variation between people. But sometimes a single change is enough to cause disease, and these changes come in a few distinct types. Let’s review them because each type breaks the instructions in a different way, and causes different types of issues.
A substitution, or point mutation, swaps one letter for another. In sickle cell disease, a single swapped letter in the gene for hemoglobin warps red blood cells into a stiff, sickle shape. Here is the twist: carrying just one copy of that same change protects against malaria, which is why it became common where malaria was widespread; an example of evolution at work. The same letter that harms when there are two copies, can protect when there is only one copy.
An insertion adds letters that should not be there. In Huntington’s disease, a short three-letter sequence is repeated far too many times, like a word jammed on copy and paste, and the surplus slowly damages the brain in adulthood.
A deletion removes letters. In cystic fibrosis, just three missing letters leave out a single building block of a crucial protein, and the result is thick mucus that clogs the lungs and digestive system.
A copy number variation changes how many copies you have of a whole gene or even a whole chromosome. An extra copy of chromosome 21 causes Down syndrome. Extra copies of a gene called HER2 drive some aggressive breast cancers.
A translocation happens when two chromosomes break and swap pieces. In chronic myeloid leukemia, parts of chromosomes 9 and 22 fuse to create an abnormal gene, BCR-ABL1, that tells blood cells to multiply out of control.
Applications: Four ways genomics is changing medicine
As our understanding has grown, four major applications have emerged.
Predicting cancer risk. Some mutations act as an early warning. A woman who inherits a faulty BRCA1 gene can face a lifetime breast cancer risk as high as roughly 70%, against about 12% for the average woman. Knowing that years or decades ahead opens the door to closer screening, preventive surgery, or risk-reducing drugs. It is the science behind Angelina Jolie’s widely publicized preventive mastectomy. But here is the crucial context: fewer than 10% of women diagnosed with breast cancer carry a BRCA1 or BRCA2 mutation. For the other 90 in 100, how we live still plays a major role.
Precision treatment. Instead of treating a cancer only by the organ where it started, doctors increasingly treat it by the specific fault driving it. Breast cancer is a good example, because it is really several different diseases. Some breast cancers are driven by a protein called HER2, which sits on the surface of cells and tells them to grow and divide. When a tumor makes far too much HER2, it grows aggressively, and a drug called Herceptin latches onto HER2 to block that signal. Other breast cancers are driven not by HER2 but by hormones such as estrogen, and those are treated with drugs that block the hormones instead. So two women with the same diagnosis on paper may receive completely different treatments, depending on what is driving the tumor. The same idea reaches beyond breast cancer. In chronic myeloid leukemia, a protein called BCR-ABL1 drives the disease, and a drug called imatinib was built to jam that exact protein, turning a once-deadly cancer into one that can often be controlled for life.
Pharmacogenomics. Give two people the same drug at the same dose, and one may do beautifully while the other suffers. Statins are a perfect example. Millions take them to lower cholesterol, and most do fine. But some people carry a common variant in a gene (SLCO1B1) that slows how quickly the body clears the drug. The statin builds up, and the risk of muscle pain and damage climbs sharply. A simple genetic test can flag this in advance, so a doctor can lower the dose or pick a different statin before the side effects ever start. That is the promise of pharmacogenomics: the right drug, at the right dose, for the right person, from the very first prescription. There is no need for the conventional trial and error approach that has been used all these years.
Inherited disorders. Conditions such as thalassemia, sickle cell disease, Duchenne muscular dystrophy, and spinal muscular atrophy can be caught through carrier screening in parents or testing in newborns, often long before a child shows a single symptom. And that timing, as the next section shows, can be the difference between a full life and a tragic one.
Genomics at scale: Screening newborns for SMA
One of the clearest examples of genomics working at scale is newborn screening for spinal muscular atrophy, or SMA. This is an area our own team has worked on directly, so I have seen up close both the challenge and the payoff.
SMA is caused by the loss of a gene (SMN1). In its severe form, it steadily destroys the motor neurons that control movement and breathing, and it can be fatal in infancy. The cruel part is the timing. By the time symptoms appear, motor neurons have already been lost, and that damage cannot be undone.
That is what makes screening at birth so valuable. Since 2022, the program in Turkey has screened more than four million newborns and identified 550 babies with SMA before symptoms began. Each was treated with gene therapy, a one-time infusion that delivers a working copy of the missing gene.
The timing is everything. Given in the first days of life, before the disease has destroyed motor neurons, this treatment changes the trajectory entirely. In studies of babies treated this early, the great majority went on to sit, stand, and walk on a roughly normal timeline, milestones that infants with the severe untreated form would never reach. It does not undo damage that has already happened, which is exactly why catching these babies at birth, rather than waiting for symptoms, is the whole point.
Driving the cost of screening down far enough to test millions of newborns is what makes a program like this possible. It is preventive medicine at its most concrete. And we at GenePath Diagnostics are very proud of this ground breaking work.
AI and genomics: Why they need each other
The last theme I want to discuss here is artificial intelligence because of the ramifications it has on scalability as well as accuracy.
Let’s start with why experts need AI. A single genome holds six billion letters. Once you are screening millions of people, no team of human specialists could ever read and interpret that much data by hand. AI can sift through it at a speed and scale no human can match, surfacing the handful of genetic variants that matter out of the millions that do not. Without AI, genomics simply cannot reach population scale.
But AI on its own is dangerous here. We have in our own lab seen AI-generated genomic reports that looked polished and authoritative, yet contained genes that do not exist, mutations that were never there, and locations that are biologically impossible. To an untrained reader, they were completely convincing. An expert caught the errors instantly. A patient making decisions about their own health would not.
That is the delicate balance. Lean too far toward pure automation and you get fast, confident, wrong answers. Rely only on human experts and you can never serve more than a fraction of the people who need it. The goal is a system where AI carries the scale and experts guard the accuracy, each covering the other’s weakness. It is the cleanest version of a lesson I expect to see across all of medicine:
AI without experts is not credible. Experts without AI are not scalable.
Final thoughts
As genomic testing becomes increasingly accessible, generating the data is no longer the hard part. The challenge is turning that data into guidance that is accurate, actionable, and trustworthy.
Understanding our DNA can help us predict disease earlier, match treatments to the individual, and in some cases act before symptoms show up. But knowing what to do with that information may matter even more than the information itself. Together, they enable preventive healthcare, which in turn should impact healthspan and longevity.
Disclaimer
Views expressed above are the author’s own.